This editorial outlines a clinical approach to patients with periodic inflammation of unknown origin despite initial rational and targeted investigation. The focus of the editorial is on the recognition and diagnosis of systemic autoinflammatory diseases (SAIDs). Although rare, SAIDs are valuable diagnoses given they carry a risk of disease-associated damage and are often treatable. The authors are from a subspecialty clinic in London, UK, which is the national referral centre for adult SAIDs. The basis of this approach is both a review of the literature and our experience from our fever clinic to which patients are referred for the consideration of a SAID diagnosis in the setting of periodic fever and inflammation.
Periodic inflammation
Fever of unknown origin (FUO) was first defined by Petersdorf and Beeson in 1961 as a temperature greater than 38.3°C on three or more occasions which remained unexplained after one week of inpatient investigation.1 This definition has been updated several times in the intervening years with advances in diagnostics.2 In our clinical practice we utilize a definition that is tailored towards a higher probability of systemic autoinflammation and occult rheumatic disease. It requires a duration of six months or more in which no diagnosis has been found by rational targeted investigation. It excludes the immunocompromised patient subgroup but includes patients presenting with inflammation of unknown origin (IUO), defined as elevated serum inflammatory markers without markedly elevated temperature (Figure 1).
Figure 1: A definition of periodic inflammation of unknown origin for use in a clinic designed to diagnose systemic autoinflammatory diseases and other rheumatic conditions
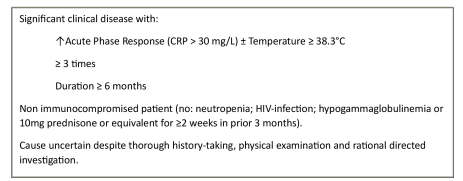
CRP = C reactive protein; HIV = human immunodeficiency virus.
The main categories of diseases found to be responsible for FUO presentations in the financially privileged countries of the northern hemisphere are: infection (20%), non-infectious inflammatory diseases (NIIDs; 25%), malignancy (10%), miscellaneous (5–10%) and unknown (35–40%).3 The major ‘miscellaneous’ cause is drug-associated fever, but others include obesity and liver cirrhosis.3 The causes underlying FUO presentations have varied over time and location. Previously, infection accounted for up to 50% of FUO in financially privileged countries and still does in the developing world (primarily caused by tuberculosis). As infection has reduced as a cause in financially privileged countries, NIIDs have correspondingly become more common.3,4 Diagnosis of an NIID is more likely with longer duration of fever/inflammation and the presence of IUO.5
The clinical significance of patients presenting with recurrent low-grade temperatures (≤38.2°C) without evidence of inflammation is unclear and how they should be approached is an issue for clinicians. One suggestion is to avoid extensive investigation in this group – in the absence of any potential diagnostic clues, symptoms or signs suggestive of significant systemic illness, only a complete blood count, inflammatory markers, and urinalysis are suggested, although our practice is to exclude connective tissue disease too.2 If these are normal, the clinician must validate the reality of the patient’s symptoms while reassuring them about the results of testing. Management can consist of symptom control, sympathetic holistic care and close follow up.2
Diagnostic process
The initial diagnostic process for periodic IUO is well described and set out in Table 1.6,7 Some caveats to this process must be noted – in adults, an accurate history of fever can be hard to elicit; a focus on rigors and night sweats can improve specificity. Conversely, in very long-standing IUO, individuals may have ‘hardened’ to their symptoms and minimize the impact, resulting in low sensitivity on screening questioning. In the authors’ experience, an example of this is the diagnosis of parents with autosomal dominant SAIDs only after their children have presented. Any concerns in an infection history should prompt referral for specialist input. It is also worth noting that the descriptions of classical rashes are based upon their appearance in Caucasians and may present differently or be absent in persons of colour.
Table 1: Initial ‘classical’ diagnostic process for periodic inflammation6,7
|
History |
|||
|
Features/symptoms |
Risk factors |
Family history |
Targeted history for occult cases |
|
Duration |
Drug history |
Suggestive features of hereditary disease |
Atypical and occult infections |
|
Age at onset |
Travel history |
Ethnicity |
Occult NIIDs: LVV, PMR, SLE |
|
Precipitating event |
Sexual history |
Consanguinity |
Serositic diseases |
|
Constitutional symptoms: fever, rigors, weightloss, night sweats |
Occupation |
|
IBD |
|
Lymphoreticular symptoms: adenopathy, tonsillitis |
Hobbies |
|
Sacroiliitis |
|
Mucocutaneous symptoms: rash, ulcers, lesions |
Vaccination history |
|
Features of endometriosis |
|
Musculoskeletal symptoms: arthritis, arthralgia, myalgia |
Antimicrobial history |
|
|
|
Serosal symptoms: pericarditis, pleuritis, abdominal |
Immunosuppresive history |
|
|
|
Luminal GI symptoms: inflammatory diarrhoea |
|
|
|
|
CNS symptoms: sensorineural hearing loss |
|
|
|
|
Physical Examination |
|
|
Purpose |
Specific systems and signs often missed |
|
Looking for pathognomonic signs |
Full skin examination for rash |
|
To direct further targeted investigations |
Examination of mucus membranes, mouth and tonsils |
|
|
Palpation of lymph nodes |
|
|
Palpation for organomegaly |
|
|
Eye examination with fundoscopy |
|
Investigations |
||
|
Obligatory tests |
Additional tests worth considering |
Cardiovascular risk factors |
|
ESR |
Procalcitonin |
BP |
|
CRP |
Serum ACE |
Lipid profile |
|
FBC and differential |
TFTs, FSH, LH |
Folate |
|
Creatinine, electrolytes, total protein |
Cryoglobulins |
|
|
ALP, AST, ALT, LDH, CK |
Fuller auto antibody screen |
|
|
ANA, RF |
C3 and C4 |
|
|
Protein electrophoresis |
ASOT |
|
|
Ferritin |
|
|
|
Three blood cultures, urine culture |
|
|
|
TB testing |
|
|
|
Microscopic urinalysis |
|
|
|
CXR, abdominal ultrasonography |
|
|
ACE = angiotensin conversion enzyme; ALP = alkaline phosphatase; ALT = alanine transaminase; ANA = anti nuclear antibody; ASOT = anti-streptolysin O titre; AST = aspartate transaminase; BP = blood pressure; C3 = complement 3; C4 = complement 4; CK = creatine kinase; CNS = central nervous system; CRP = C reactive protein; CXR = chest X-ray; ESR = erythrocyte sedimentation rate; FBC = full blood count; FSH = follicle-stimulating hormone; GI = gastrointestinal; IBD = inflammatory bowel disease; LDH = lactate dehydrogenase; LH = luteinising hormone; LVV = large vessel vasculitis; MSK = musculoskeletal; NIIDs = non-infectious inflammatory diseases; PMR = polymyalgia rheumatica; RF = rheumatoid factor; SLE = systemic lupus erythematosus; TB = tuberculosis; TFTs = thyroid function tests.
A trial of cessation of any potential culprit medications for drug-induced fever is advisable. Drug-induced fevers have a median onset of 7–10 days post medication commencement, but there can be very marked variation in timing. Some of the common culprit medications are antibiotics (beta-lactams and sulphonamides), allopurinol, anticonvulsants (phenytoin and carbamazepine), antiarrhythmics (procainamide and quinidine), and antineoplastic agents.8
FDG-PET/CT is now established as the advanced imaging modality of choice for FUO, and is often utilised by our clinic.9 In a meta-analysis, FDG-PET/CT had high sensitivity (83%) and moderate specificity (64%) for identifying the underlying diagnoses causing FUO.3 The diagnostic yield of 54% indicates that over half of the patients undiagnosed following initial investigation were guided to a final diagnosis by FDG-PET/CT.3 Biopsy is indicated only when targeted by potential diagnostic clues. Protocol bone marrow biopsies have a low diagnostic pick up rate and are not recommended unless specifically looking for a haematological malignancy or myelodysplasia, or investigating an infectious disease which resides in bone marrow.10
Our practice is to collect serial fortnightly inflammatory markers, C reactive protein and serum amyloid A, over at least 3 months in all patients with IUO. These specific markers are preferred due to their short half-lives and rapid response to the presence or removal of inflammation.11 It is our experience that in patients with isolated fever, persistently normal inflammatory markers can provide useful reassurance, and in patients with episodic inflammation, serial bloods are more informative than isolated clinic blood draws. Certain patterns of inflammation, as described in Figure 2, can aid diagnosis.
Figure 2: Characteristic patterns of inflammation from fortnightly CRP measurement
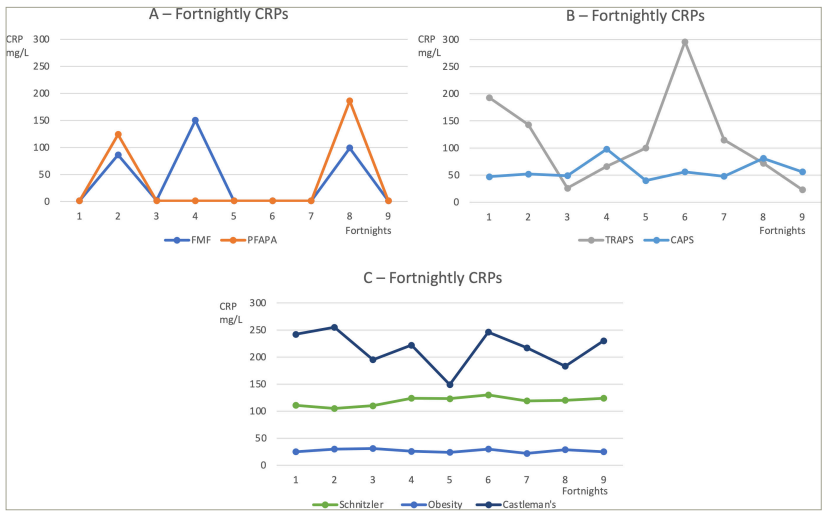
Example animations of common patterns of inflammation. (a) – periodic inflammation with complete normalization in between attacks. Seen in milder FMF and in PFAPA. (b) – Persistent inflammation with flares. Seen in TRAPS, and, to a lower extent, in CAPS. (c) – Fixed inflammation. High-grade fixed inflammation in Castleman’s disease and to a less severe extent in Schnitzler syndrome. Low-grade fixed inflammation in obesity.
CAPS = cryopryrin associated periodic syndrome; CRP = C-reactive protein; FMF = familial Mediterranean fever; PFAPA = periodic fever, aphthous ulcers, pharyngitis and adenopathy; TNF = tumour necrosis factor; TRAPS = TNF-receptor associated periodic fever syndrome.
SAID remains a rare cause of IOU, but SAIDs are extremely high-value diagnoses because they carry risks of disease-associated damage if untreated and are often amenable to effective long-term therapy. There are published criteria to guide the decision to order genetic testing for SAIDs.12–15 Using classification criteria prior to genetic testing allows the selection of the simplest genetic test available to answer the specific clinical question and can support interpretation of equivocal results. Our practice is to use a next-generation sequencing (NGS) panel of 24 selected SAID genes in all patients with IUO except in those where there is a clinical suspicion for a distinct single SAID, such as familial Mediterranean fever (FMF), where single-gene Sanger sequencing is used.16 Our real-world experience has been that the NGS panel returns a variant of uncertain significant in 60% of patients.
When diagnostic work-up fails, there is a role for research-led investigation of individuals or families in whom there is a high suspicion of SAID. This can involve techniques such as whole exome sequencing, whole genome sequencing and cytokine panels.15 The description of VEXAS (vacuoles, E1 enzyme, x-linked, autoinflammatory, somatic) syndrome is an example of this process – a research-based theory regarding the likely pathogenic outcome of somatic mutations in the UBA1 gene was applied to the genetic data of many patients with unspecified inflammatory disease. Through this genotype-driven approach, a clinical phenotype was identified.17
High-value non-SAID diagnoses
In our experience, the malignancies which most closely mimic SAIDs and can evade early detection are Castleman’s Disease, Hodgkins and non-Hodgkins lymphomas, and renal cell carcinoma. These have all been associated with elevated levels of interleukin (IL)-6, and this may be the driver of their febrile presentation.18 Clinicians are understandably concerned about possible aggressive malignancies, such as acute leukaemia or high-grade lymphomas; however, these usually present with a rapid trajectory and with several diagnostic clues which lead to accurate diagnosis.19
The most common NIID diagnoses for IUO are: adult-onset Still’ disease (AOSD) (20%), large vessel vasculitis (10%), systemic lupus erythematosus (10%), anti-neutrophil cytoplasm antibody (ANCA)-associated vasculitis (7%), and polymyalgia rheumatica (7%).5 An index of suspicion must be maintained for atypical infections and for uncommon presentations of the more common NIIDs, such as occult inflammatory bowel diseases and sacroiliitis.
Systemic autoinflammatory diseases
In 2017, of 273 new referrals at our national referral clinic for adult SAID, 25% received a diagnosis of a monogenic SAID, primarily FMF, cryopryrin-associated periodic syndrome (CAPS) and tumour necrosis factor receptor-associated periodic fever syndrome (TRAPS). Most of these patients had life-long disease and missed diagnoses in childhood. A minority had adult-onset disease due to milder late-onset symptoms or somatic mosaicism. The recent discovery of VEXAS syndrome has now broadened the scope of adult-onset monogenic SAID.17
Of our patients, 12% received a diagnosis of a specific non-monogenic SAID: either AOSD, Schnitzler syndrome, PFAPA (periodic fever, aphthous ulcers, pharyngitis and adenopathy), or idiopathic recurrent pericarditis (IRP). These are high-value diagnoses as they have effective therapies available, as outlined in Table 2.20–22 A further 13% had a suspected SAID, but no specific diagnosis and were classed as undifferentiated SAID (USAID). There is a recognition that these non-genetic diagnoses are useful groupings for guiding management, but may in turn prove to be incorrect as we gain more knowledge.
Table 2: High-value non-genetic systemic autoinflammatory disease diagnoses with effective therapy available
|
Disease |
Onset |
Diagnostic clues |
Treatment |
|
AOSD |
Adult (sJIA in children) |
Yamaguchi criteria20:* |
Anti IL-1 |
|
Major criteria: |
Corticosteroids |
||
|
Fever ≥39°C (≥1 week) |
NSAIDs |
||
|
Arthralgia (≥2 weeks) |
|
||
|
Typical rash |
|
||
|
Leukocytosis (≥10,000 /mm3) with ≥80 % granulocytes |
|
||
|
Minor criteria: |
|
||
|
Sore throat |
|
||
|
Lymphadenopathy and/or splenomegaly |
|
||
|
Liver dysfunction |
|
||
|
Negative RF and ANA |
|
||
|
Exclusion criteria: infections, malignancy, rheumatic diseases |
|
||
|
Diagnosis:≥5 criteria, including ≥2 major criteria |
|
||
|
PFAPA |
Most commonly children ages 1-4 years, some adult onset |
Periodic fever: usually lasts 3-5 days and predictably repeats every 3-4 weeks |
Colchicine |
|
Aphthous ulcers: small, shallow and usually resolve quickly |
Stat. prednisolone |
||
|
Pharyngitis: with or without exudate |
Tonsillectomy |
||
|
Adenopathy: usually cervical and short lived |
|
||
|
Arthralgia very frequent |
|
||
|
Not all features present in one attack, but all occur over disease course |
|
||
|
Schnitzler Syndrome |
Adult |
Strasbourg criteria21: |
Anti IL-1 |
|
Urticarial rash, monoclonal IgM component, and ≥2 of the following: |
|||
|
Fever |
|||
|
Arthralgia/arthritis |
|||
|
Bone pain |
|||
|
Palpable lymph nodes and/or liver or spleen enlargement |
|||
|
Elevated erythrocyte sedimentation rate |
|||
|
Leukocytosis |
|||
|
Abnormal findings on bone morphologic investigations |
|||
|
IRP |
Any age |
European Society of Cardiology criteria22: |
Colchicine |
|
≥2 episodes of pericarditis with at least a 4-6 week symptom-free interval |
Anti IL-1 |
||
|
Episode must be confirmed by presence of ≥2 of the following: |
NSAIDs |
||
|
Chest pain, pericardial rub, consistent ECG changes, new or worsening pericardial effusion. |
|
||
|
Supportive features: elevated inflammatory markers, CT/MRI support |
|
||
|
Exclusion criteria: infection, malignancy, rheumatic disease, cardiac trauma |
|
*Note there are other diagnostic criteria available for AOSD, however these are the most commonly used/recognised criteria.
ANA = anti nuclear antibody; AOSD = adult-onset Still disease; ECG = electrocardiogram; IgM = immunoglobulin M; IL-1 = interleukin 1; IRP = idiopathic recurrent pericarditis; NSAIDs = non-steroidal anti-inflammatory drugs; PFAPA = periodic fever, aphthous ulcers, pharyngitis and adenopathy; RF = rheumatoid factor; sJIA = systemic juvenile idiopathic arthritis; Stat = statim.
The authors’ opinion is that a trial of therapy is warranted for suspected SAID, but this relies upon a robust predefinition agreed upon by the clinician and the patient as to what constitutes clinical success and when ineffective treatments should be stopped. Caution should be taken with corticosteroids as the risk of iatrogenic harm is high. Our first-line choice is a trial of therapeutic dose colchicine as outlined in Figure 3. Anti IL-1 biological treatments can also be very effective, if they are able to be accessed.
Figure 3: Authors’ recommendations for trials of therapeutic dose colchicine
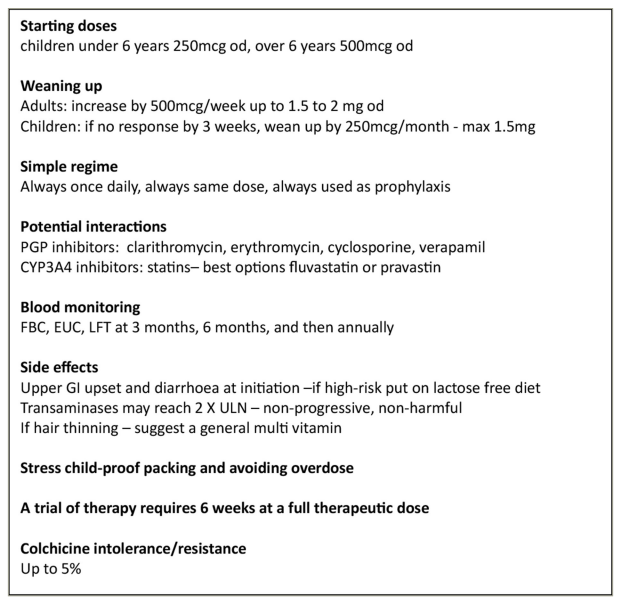
OD = once daily; PGP = P glycoprotein; CYP = cytochrome P450; FBC = full blood count; EUC = electrolytes, urea and creatinine; LFT = liver function tests; GI = gastrointestinal; ULN = upper limit of normal.
A baseline review of cardiovascular disease (CVD) risk factors should be sought and actively managed in all individuals with prolonged inflammation.23 CVD is a leading cause of mortality and morbidity in many inflammatory conditions.
No diagnosis
In up to 50% of patients with periodic inflammation, no diagnosis is made.7 In these cases, invasive tests and radiation-based imaging should not be repeated unless new diagnostic clues emerge, or the patient deteriorates. Stable patients have a good prognosis and should be reassured and NSAIDs can be used for symptom control. Mortality rates are extremely low and up to 95% will experience spontaneous resolution of fevers over extended follow-up.24,25
Conclusions
Patients with periodic inflammation who have not been diagnosed by an initial rational and targeted investigation process pose a clinical conundrum. In this article, we have set out our approach to these patients, with a focus upon how to diagnose SAIDs. This approach involves seeking high-value diagnoses via genetic testing and recognition of specific non-genetic SAIDs. Empiric trials of therapy are warranted when SAIDs are suspected but not confirmed. Not achieving a final diagnosis is very common, and the clinician’s role is to help manage the uncertainty around this.